Standards for Continuing Certification
Effective January 1, 2024
Approved by the Board of Directors of the American Board of Medical Specialties (ABMS) on October 29, 2021
Introduction | General Standards | Professional Standing and Conduct | Lifelong Learning | Improving Health and Health Care | Appendices
Introduction
The American Board of Medical Specialties (ABMS) board certification is a program of rigorous, continuous professional assessment and development. It begins with initial certification after the completion of residency training and is sustained through a process of continuing certification. Continuing certification is an ongoing program that embodies a lifelong dedication to professional growth and excellence as well as a commitment to the ABMS/Accreditation Council for Graduate Medical Education (ACGME) Core Competencies.
These new “Standards for Continuing Certification” (Standards) promote the design of integrated, specialty-specific programs by Member Boards that support an individual physician’s or medical specialist’s (i.e., diplomate’s) continuing professional development. The Standards also maintain the social contract between the medical profession and the public to improve the quality, safety, and value of health care. Taken together, the Standards provide a comprehensive framework for Member Boards to design certification programs that meaningfully engage diplomates in activities relevant to their practice.
Read more Introduction
Professionalism is central to self-regulation; so it is to board certification. To honor medicine’s social contract and uphold the public’s trust, individual diplomates are expected to affirm, reaffirm, and demonstrate their dedication through the highest professional conduct in their interactions with patients, families, and all others in the health care environment. This entails a personal commitment to the welfare of patients and collective efforts to improve the health care system for the benefit of society. Professionalism is a core element in the design and implementation of each Member Board’s continuing certification program, thus communicating its centrality and cultivating professional behavior in all diplomates.
ABMS and its Member Boards have a unique role in professional self-regulation in the U.S. The ABMS mission is to serve the public and the medical profession by improving the quality of health care through setting professional standards for lifelong certification in partnership with Member Boards. ABMS assists Member Boards in their development and use of assessment and professional standards for the certification of physicians and medical specialists. The elements of a continuing certification program complement and are integrated with one another through their design and function.
Member Boards’ certification programs serve patients, families, and communities by providing diplomates with specialty-specific credentials on which the public and those acting on its behalf can rely. Member Boards’ certification programs ensure that diplomates are in good professional standing, are keeping up to date with advances in medical knowledge, and are working to improve themselves, their colleagues, and the systems in which they work. ABMS Member Boards strive to develop programs that integrate seamlessly to support a diplomate’s practice. Member Boards work collaboratively with key stakeholders — specialty societies, associations, patient advocacy groups, and others — to ensure that high-priority population and public health needs are addressed and that advances in the specialty are reflected in their continuing certification programs.
Organization of this Document
The Standards document has been organized into the following groupings: General Standards, Professional Standing and Conduct, Lifelong Learning, and Improvement in Health and Health Care. These Standards represent an evolution of previous continuing certification standards and retain the central elements of the ABMS/ACGME core competencies.
These Standards guide the design of Member Board continuing certification programs. Each Member Board meets each requirement in a manner consistent with the spirit of the Standard and in a fashion consistent with its specialty. Each Standard has an associated commentary. Commentaries do not specify additional requirements, but they provide rationale, context, and address additional considerations. In most places, the commentaries also reflect the recommendations of the Continuing Board Certification: Vision for the Future Commission (see Appendix II) to increase consistency across Member Boards and to clarify when specialty-specific variation is needed.
The Standards provide a comprehensive framework for Member Boards to design certification programs that ensure diplomates have the knowledge, judgment, and skills to provide excellent patient care.
General Standards
Preamble
The General Standards guide the continuing certification programs of the 24 ABMS Member Boards. These standards provide a framework for improving patient care through a meaningful process of ongoing professional development and assessment that is aligned with other professional expectations and requirements.
Requirements for Member Boards
1. Program Goals: Member Boards must define goals for their continuing certification program that address the overarching themes in the Introduction and each of the subsequent standards in this document. [Read Commentary]
Commentary
Program elements should be designed to achieve the goals of the program, highlight the boards’ unique role as an assessment organization, lessen diplomate burden, support diplomates in their professional obligation to keep up to date with advances in medical knowledge, and continually improve themselves, their colleagues, and the systems in which they work. The goals and components of continuing certification programs should be clearly communicated and available on Member Board websites for stakeholders, which includes the public, diplomates, and credentialers.
2. Requirements for Continuing Certification: Member Boards must define the requirements and deadlines for each component of their integrated continuing certification program. [Read Commentary]
Commentary
Both participation and performance requirements for each component must be clearly specified along with the intervals at which they must be completed. Any decision on the certificate status of a diplomate by a Member Board must be based on each component of their integrated continuing certification program.
Member Boards may make allowances for diplomates with extenuating circumstances who cannot complete requirements to stay certified according to established timelines. Appropriate procedures to ensure due process regarding Member Board decisions must be in place and clearly communicated to diplomates as part of diplomate engagement. Member Boards should have a process to verify attestation for participation standards.
3. Assessment of Certification Status: Member Boards must determine at intervals no longer than five years whether a diplomate is meeting continuing certification requirements to retain each certificate. [Read Commentary]
Commentary
Assessment of certification status on a frequent interval provides the public and credentialers trusted information about the diplomate; therefore, Member Boards may make certification decisions on a more frequent interval than five years. Policies that specify the requirements for certification and the relevant periodicity will be established by each Member Board. These policies require a decision to determine a diplomate’s certificate status (e.g., certified, not certified) at the established interval.
The components utilized to make a certification decision in the board-determined interval may vary (e.g., knowledge assessment, case logs, peer review, improving health and health care activity). Member Boards may have some components of their continuing certification process that extend beyond five years.
4. Transparent Display of Certification History: Member Boards must publicly display and clearly report a diplomate’s certification status and certification history for each certificate held. Member Boards must change a diplomate’s certificate(s) status if any requirements (either a performance or participation requirement) in their continuing certification program are not met. Changes in the status of a certificate must be publicly displayed, including any disciplinary status. Member Boards must use common categories for reporting the status of certificates, with such categories being defined, used, and publicly displayed in the same way. [Read Commentary]
Commentary
Member Boards have an obligation to the medical community and the public to display on their respective websites and/or the ABMS Certification Matters website, the certification status and history for each diplomate including the date of initial certification, whether the diplomate is certified, and whether the diplomate is participating in continuing certification.
5. Opportunities to Address Performance or Participation Deficits: Member Boards must provide diplomates with opportunities to address performance or participation deficits prior to the loss of a certificate. Fair and sufficient warning, determined by each Member Board, must be communicated that a certificate might be at risk. [Read Commentary]
Commentary
Diplomates should receive early notice about the need to complete any component of the continuing certification program. Diplomates at risk for not meeting a performance standard should be notified of their deficit along with information about approaches to meet the requirements. Member Boards should collaborate with specialty societies and other organizations to encourage the development of resources to address performance deficits.
The timeline to address deficits should not extend the time a diplomate has to complete requirements (i.e., deficits must be addressed within the cycle they are due). If a diplomate chooses not to address their deficits or is unsuccessful in doing so, the diplomate should be notified of the potential for the loss of certification.
6. Regaining Certification: Member Boards must define a process for regaining certification if the loss of certification resulted from not meeting a participation or performance standard. [Read Commentary]
Commentary
A pathway should be available for physicians and medical specialists to regain certification following loss of certification after a lack of participation in a continuing certification program or not meeting the performance standard.
7. Program Evaluation: Member Boards must continually evaluate and improve their continuing certification program using appropriate data that include feedback from diplomates and other stakeholders. [Read Commentary]
Commentary
It is crucial for Member Boards to evaluate their continuing certification program on an ongoing basis using a variety of metrics to guide enhancements to their program. Aspects of program evaluation should include assessing diplomate experience, the value of the program to diplomates, and whether diplomates are meeting the Member Board’s objectives. Feedback from other certification stakeholders — professional societies, credentialers, hospitals and health systems, patients, and the public — should also be considered.
8. Holders of Multiple Certificates: Member Boards must streamline requirements for diplomates who hold multiple certificates, to minimize duplication of effort and cost. [Read Commentary]
Commentary
Diplomates who hold multiple specialty and/or subspecialty certificates from one or more Member Boards could have duplicative requirements to maintain all certificates. Member Boards should avoid redundancy of requirements of programs for their diplomates maintaining multiple certificates from their board (e.g., Lifelong Learning credit for participation in longitudinal assessment and improving health and health care credit for quality improvement efforts).
Similar processes should be incorporated to offer reciprocity of credit for diplomates with multiple certificates held across Member Boards (e.g., Lifelong Learning credit for participation in longitudinal assessment and improving health and health care credit for quality improvement efforts).
9. Diplomates Holding Non-time-limited Certificate: Member Boards must have a process by which non-time-limited certificate holders can participate in continuing certification without jeopardizing their certification status. [Read Commentary]
Commentary
Member Boards must have a process for diplomates with non-time-limited certificates to apply for and participate in their continuing certification programs. Certificates for non-time-limited certificate holders should not be at risk for failure to meet continuing certification requirements if the diplomate participates in continuing certification; however, Member Board professional standing and conduct standards must be upheld by all certificate holders in order to remain certified.
Professional Standing and Conduct
Preamble
Professionalism is central to public trust in diplomates, certification, and the medical profession. Professional standing refers to maintaining high standards of professional conduct through which diplomates carry out their clinical responsibilities ethically, professionally, and safely. In the absence of workplace behavior measurement, we define “professional standing” in terms of the absence of actions by regulatory authorities that signify a breach of professional norms.
Maintenance of an unrestricted medical license is fundamental to professional standing. Medical licensure is a legal and regulatory process that differs based on regional statutes and regulatory customs. Some licensure actions may not reflect a lack of professionalism, and some unprofessional behavior may not trigger a licensure action. ABMS and the Member Boards will develop approaches to evaluate professional standing and conduct using multiple sources.
Requirements for Member Boards
10. Review of Professional Standing: Primary Source Verification of unrestricted licensure must occur annually. In addition, Member Boards must have a mechanism to identify and review information regarding licensure in every state in which the diplomate holds a medical license. Any actions by other authorities that signal a violation of the Member Board’s professionalism policies that become known by a board must also be reviewed. [Read Commentary]
Commentary
Credentialers and the public rely on ABMS and its Member Boards to ensure that diplomates meet high standards of professionalism. Member Boards rely on state medical licensing boards for primary evidence that diplomates maintain good standards of professional conduct, and expect medical licenses held by diplomates to be unrestricted. On a timely basis, Member Boards are expected to review available information, including restrictions forwarded to the Member Board, and take appropriate action to protect patient safety and the trustworthiness of ABMS board certification. Member Boards are expected to distinguish between material actions and actions that are administrative rule violations that do not threaten patient care or that are being appropriately monitored and resolved by the regulatory authority.
- To ensure diplomates are in good standing with their licensing board(s), ABMS will facilitate Primary Source Verification of unrestricted licensure with a seamless and efficient mechanism through which Member Boards can easily identify restrictions on a diplomate’s medical license.
- Mechanisms such as the ABMS Disciplinary Action Notification Service reports may assist Member Boards in continually monitoring any actions taking place between annual Primary Source Verification of licensure.
- Member Boards may choose to use additional methods to evaluate professional standing.
- Member Boards must effectively communicate the expectations and process for diplomate self-reporting of any changes in professional standing and the implications for failing to do so.
11. Responding to Issues Related to Professional Standing and Conduct: Member Boards must have policies on professional standing and conduct that define the process for reviewing and taking action on the information that reflects a violation of professional norms. Policies should be communicated to diplomates and available on Member Board websites. [Read Commentary]
Commentary
Member Board policies on professional standing and conduct are to be made readily accessible to diplomates and the public. These policies ensure that:
- Material actions that may imperil a diplomate’s certificate status are clearly defined (g., disciplinary actions against a license, criminal convictions, incidents of sexual misconduct);
- The facts and context of each action are considered before making any change in a diplomate’s certification status;
- Appropriate procedures to ensure due process are in place and clearly articulated to diplomates; and
- There is a clearly outlined process for diplomates to regain a revoked certificate if they are eligible to do so.
When disciplinary actions are reported, Member Boards should review each instance in which an action has been taken against a diplomate’s license (e.g., revoked, suspended, surrendered, or had limitations placed) to determine if there has been a material breach of professional norms that may threaten patient safety or undermine trust in the profession and the trustworthiness of certification.
Actions against a medical license should not automatically lead to actions against a certificate without reviewing the individual facts and circumstances of the situation. A change in certificate status should occur when the diplomate poses a risk to patients or has engaged in conduct that could undermine the public’s trust in the diplomate, profession, and/or certification. This standard for professional standing and conduct means that the loss of a certificate can result from issues that fall short of a licensure action. Conversely, some licensure actions may not warrant a change in certificate status. For example, there are instances where restrictions placed on a diplomate’s license do not reflect professionalism concerns or threaten patient safety (e.g., restrictions due to physical limitations or administrative rule violations). Some restrictions are self-imposed while some relate to administrative infractions that, while serious, may not be viewed as a breach of professional norms.
Member Boards are not investigatory bodies, but they are expected to weigh available evidence and render an informed judgment with due process. Member Boards should consider permitting a diplomate to retain a certificate when the diplomate has been successfully participating in physician health programs or other treatment programs recognized by the state medical board.
Finally, when a Member Board takes action on the certification status of a diplomate who holds certificates from multiple Member Boards, the Member Board must work with ABMS to notify other Member Boards of the action taken.
Lifelong Learning
Preamble
The certification process incorporates an independent, validated “assessment of learning” to determine that the diplomate has the knowledge, judgment, and skills to provide safe and effective patient care independently. Achieving certification assures the profession and the public that a diplomate meets the standards of the specialty. It is incumbent upon the Member Board to specify its lifelong learning objectives and to assess whether those objectives have been met.
Continuing certification programs have a dual purpose: (1) to assure the public that the diplomate continues to meet the standards of the specialty, and (2) to assist diplomates in keeping up with the evolving standards of practice in the specialty. Accordingly, continuing certification programs should include “assessment for learning” to assist diplomates in staying up to date with new, rapidly changing developments in the specialty while concurrently administering assessments that provide a fair, valid, and reliable “assessment of learning.” Diplomates have a professional duty to remain current in the knowledge, judgment, and skills of the specialty by meeting a performance standard. Member Boards have a responsibility to determine whether a diplomate has met that performance standard.
Requirements for Member Boards
12. Program Content and Relevance: Member Boards’ continuing certification programs must balance core content in the specialty with practice-specific content relevant to diplomates. [Read Commentary]
Commentary
A continuing certification program should reflect the general scope of practice encompassed by a certificate as defined in collaboration with specialty societies, as well as the specific scope of diplomate’s practice. To a reasonable degree, customization of required content should occur to enhance clinical relevance of certification.
13. Assessments of Knowledge, Judgment, and Skills: Member Boards must assess whether diplomates have the knowledge, clinical judgment, and skills to practice safely and effectively in the specialty. Member Boards must offer assessment options that have a formative emphasis and that assist diplomates in learning key clinical advances in the specialty. [Read Commentary]
Commentary
Assessments should integrate learning opportunities and provide feedback that enhances learning.
Member Boards may choose to offer point-in-time, secure assessments for diplomates who prefer this approach, provided that the Member Board can give useful feedback to guide diplomate learning.
14. Use of Assessment Results in Certification Decisions: Member Boards’ continuing certification assessments must meet psychometric and security standards to support making consequential, summative decisions regarding certification status. [Read Commentary]
Commentary
Performance on continuing certification assessments should contribute to making certification decisions when assessment is a component of the decision matrix. Continuing certification programs must provide sufficient information upon which to base a decision about a diplomate’s certification status. Member Boards should ensure that subject matter experts engaging in assessment development are clinically active.
In order for users to have confidence in the value of the certificate, sufficient psychometric standards must be met for reliable, fair, and valid assessments to make a consequential (summative) decision. Security methods must be used to determine the identity of the certificate holder while preserving assessment material without creating unnecessary burden for participating diplomates.
15. Diplomate Feedback from Assessments: Member Board assessments must provide personalized feedback that enhances learning for diplomates. [Read Commentary]
Commentary
A Member Board should provide specific, instructive feedback to each diplomate that identifies their knowledge gaps on assessments. Feedback should also inform any risk to loss of certification.
Member Boards should work with specialty societies and other stakeholders to identify educational resources that address knowledge and skills gaps, and to inform diplomates about these. Member Boards should also work with specialty societies to allow diplomates to share Member Board assessment data to support personalized learning plans implemented by specialty societies.
16. Sharing Aggregated Data to Address Specialty-based Gaps: Member Boards must analyze performance data from their continuing certification program to identify any specialty-based gaps. Aggregated identified gaps should be shared with essential stakeholders, including diplomates, for the development of learning opportunities. [Read Commentary]
Commentary
An analysis of performance data allows identification of specialty-specific knowledge gaps. By sharing these data, educational organizations can create targeted learning resources for the benefit of the specialty.
Summary data should only be shared with essential stakeholders, such as specialty societies, who require the information for nonprofit service to the profession. Member Boards should collaborate with specialty societies in a continual and timely manner to address major public health needs and frequently occurring deficits, engaging specialty societies in the bidirectional communication necessary for further identification and prioritization of gaps.
17. Lifelong Professional Development: Member Boards’ continuing certification programs must reflect principles of Continuing Professional Development (CPD) with an emphasis on clinically oriented, highly relevant content. [Read Commentary]
Commentary
Continuing certification should increase a diplomates’ knowledge, skills, and abilities that result in the provision of safe, high-quality care to patients. CPD activities must be of high quality and free of commercial bias.
Member Boards should work with stakeholders to help diplomates identify relevant, high-quality activities and report completion with minimal administrative burden.
Improving Health and Health Care
Preamble
Diplomates are intrinsically motivated to provide safe, effective, efficient care to patients, families, and communities. Professional norms expect that diplomates will work to improve their skills and work collaboratively with others to improve the systems in which they work.
Member Boards should align requirements with diplomates’ daily practices and required activities that may be required by hospitals, health systems, payers, and other groups. In this way, the diplomates can apply their improvement activities to multiple purposes.
Recognizing that diplomates differ in their knowledge and experience with improvement, Member Boards should take a developmental approach to the implementation of these standards. It is reasonable to expect that the rigor of these requirements will evolve as diplomates progress in their careers and as systems that support the work of quality and safety mature.
Through these standards, Member Boards can be part of the solution in responding to the persistent and significant quality gaps that exist.
Requirements for Member Boards
18. Quality Agenda: In collaboration with stakeholder organizations, Member Boards must facilitate the process for developing an agenda for improving the quality of care in their specialties. One area of emphasis must involve eliminating health care disparities. [Read Commentary]
Commentary
Member Boards are expected to support a quality agenda in alignment with their specialty-at-large.
Member Boards must collaborate with key organizations, including specialty societies and other quality organizations, to identify areas in which patient care can be improved, review the areas, and define strategies to improve care. To support a quality agenda, Member Boards should use the common framework developed by the Institute of Medicine (IOM) for safe, timely, effective, efficient, equitable, and patient-centered care.
19. Engagement in Improving Health and Health Care: Member Board continuing certification programs must commit to helping the medical profession improve health and health care by: [Read Commentary]
- Setting goals and meeting progressive participation metrics that demonstrate an ever-increasing commitment towards having all diplomates engaged in activities that improve care;
- Recognizing the quality improvement expertise of partner organizations and seeking collaborative opportunities for diplomate engagement with efforts to improve care through a variety of existing efforts;
- Working with partner organizations, including medical specialty societies, to create systems (e.g., data transfer process), for diplomates engaged in the organizations’ quality improvement activities to seamlessly receive credit from the Member Boards; and
- Modeling continuous quality improvement by evaluating methods and sharing best practices for program implementation and diplomate engagement.
Commentary
Wherever possible, Member Boards should align their expectations to existing performance measurement, quality reporting, and quality improvement efforts.
Member Boards should work with specialty societies and other stakeholders to ensure that opportunities exist for diplomates in all practice settings and in non-clinical roles (e.g., educator, researcher, executive, or advocate).
Progressive participation goals may be appropriate for those Member Boards that are developing new programs or revising current programs.
Appendix I: Glossary
ABMS/ACGME Competencies
The Six Core Competencies, adopted by the American Board of Medical Specialties (ABMS) and Accreditation Council for Graduate Medical Education (ACGME) in 1999, are recognized as integral to quality patient care[1], and are, as follows:
- Practice-based Learning and Improvement refers to the diplomate’s ability to investigate and evaluate patient care practices, appraise and assimilate scientific evidence, and improve the physician’s practice of medicine, the collaborative practice of medicine, or both.
- Patient Care and Procedural Skills refers to the diplomate’s use of clinical skills and ability to provide care and promote health in an appropriate manner that incorporates evidence-based medical practice, demonstrates good clinical judgment, and fosters patient-centered decision-making.
- Systems-based Practice refers to the diplomate’s awareness of, and responsibility to, population health and systems of health care. The physician should be able to use system resources responsibly in providing patient care (e.g., good resource stewardship, coordination of care).
- Medical Knowledge refers to the diplomate’s demonstration of knowledge about established and evolving biomedical, clinical, and cognate sciences, and the application of these sciences in patient care.
- Interpersonal and Communication Skills refers to the diplomate’s demonstration of skills that result in effective information exchange and partnering with patients, their families, and professional associates (e.g., fostering a therapeutic and ethically sound relationship , using effective listening skills with nonverbal and verbal communication; being mindful of health literacy; and working effectively in a team both as a team member and as a team leader).
- Professionalism refers to the diplomate’s demonstration of a commitment to carrying out professional responsibilities, adhering to ethical principles, applying the skills and values to deliver compassionate, patient-centered care, demonstrating humanism, being sensitive to diverse patient populations and workforce, and practicing wellness and self-care.
ABMS Member Board
Medical Specialty Board expressly recognized and approved by ABMS as a Member by virtue of its meeting, from time to time, the ABMS’ criteria for certification and/or Maintenance of Certification/Continuing Certification of physicians and/or medical specialists within that specialty.
ABMS standards and requirements
Standards are requirements for each ABMS Member Board for the design of its continuing certification program. Each Member Board should meet each requirement in a manner consistent with the spirit of the standards and in a fashion consistent with its specialty.
Board certification
Board certification is a program of continuing, rigorous professional assessment and development. It begins with initial certification and is sustained as a process of continuing certification, which exemplifies a lifelong dedication to professional growth, excellence in the practice of medicine in the specialty, and a commitment to the ABMS/ACGME Core Competencies.
Certification history
Certification history includes the date of initial certification, current certification status, status of participation in continuing certification, and verification dates.
Competence
The array of abilities across multiple domains or aspects of physician performance in a certain context. Statements about competence require descriptive qualifiers to define the relevant abilities, context, and stage of training. Competence is multi-dimensional and dynamic. It changes with time, experience, and setting.[2]
Continuing Professional Development
Continuing professional development includes all activities that doctors undertake, formally and informally, including but not limited to continuing medical education, in order to maintain, update, develop and enhance their knowledge, skills, and attitudes in response to the needs of their patients.[3]
Diplomate
A diplomate is a physician or medical specialist who is board certified by one or more of the 24 ABMS Member Boards for demonstrated knowledge in a particular medical specialty or subspecialty. Once board certified, the individual may be referred to as a diplomate of the board.
ABMS Disciplinary Action Notification Service
A data service offered by ABMS to its Member Boards and contains disciplinary order details from 70 State medical boards on 200+ disciplinary action types with order dates. It is delivered on-demand via batch reports and daily push-alerts. It is based on the daily person-to-person sync with the Federation of State Medical Boards and does not include licensure data.
Formative assessment
Assessment of a diplomate with the primary purpose of providing feedback for learning and improvement and for reinforcement of skills and behaviors that meet established criteria and standards without passing a judgment in the form of a permanently recorded overall score.[4]
Improving Health and Health Care
Improving Health and Health Care is the process through which diplomates (1) improve their clinical performance and skills, (2) collaborate with others to optimize patient outcomes, reduce harm from care, or eliminate low-value care.
ABMS Licensure Information Delivery Service
A data service offered by ABMS to its Member Boards that contains license number, state of licensure, and dates of issue and expiration for 12 license types (such as Administrative, Supervising Physician, Temporary, Training, etc.) along with biographical data to review what ABMS used for a person-to-person match with the Federation of State Medical Boards (FSMB). It is delivered monthly via reports that are compiled by ABMS on data validated by FSMB. It is based on the daily person-to-person sync with FSMB and includes active licenses only.
Licensure standards
The requirements for physicians and medical specialists regarding professional licensure to practice general medicine, a particular type of medicine (e.g., Administrative Medicine, Academic Medicine, etc.), or a medical specialty in the United States, its territories, or Canada, as outlined in the ABMS Professional Standing Policy.
Longitudinal assessment
Longitudinal assessment applies adult learning principles (repetition and relevance) and modern technology to diplomate and medical specialist testing to promote learning, retention, and transfer of information to patient care situations.[5]
Material (actions, restrictions, lapses)
Material refers to actions, restrictions, or lapses that reflect a risk to patients or that may undermine public trust in the profession.
National Academy of Medicine Framework
Framework for a set of aims for 21st Century healthcare systems published by the Institute of Medicine in Crossing the Quality Chasm: A New Health System for the 21st Century, 2001 (now the National Academy of Medicine).[6]
Opportunities to address performance or participation deficits
Identifies a deficit prior to any changes in the certification status and allows a diplomate to address the deficit.[7]
Participating in continuing certification status
The status means that a diplomate is registered for and satisfying the relevant requirements of the ongoing program of professional development, quality improvement, and assessment activities identified by the Member Board for the specialty and/or subspecialty.
Participation standards
Thresholds for diplomate participation specified by a Member Board for components of their continuing certification program.
Performance standards
Thresholds for diplomate performance specified by a Member Board for components of their continuing certification program that demonstrate achievement of board standards for knowledge, judgment, and skills.
Physicians and medical specialists
A physician or medical specialist who has successfully completed training in a residency in a specialty or fellowship in a subspecialty of medicine whom a Member Board deems eligible for certification, continuing certification/maintenance of certification, or some other credential issued by the Member Board.
Portfolio of certification components
A portfolio is a compilation of a diplomate’s learning activities and assessment data over a period of time. Many portfolios are active databases that allow a diplomate to define and track their scope of practice and gather and track process and patient outcomes data. A portfolio may support continuing certification by providing multiple observations of a candidate’s professionalism, learning self-assessment, objective assessments, and quality improvement activities.[8]
Primary source verification
Verification of a specific credential to determine the accuracy of the qualifications of an individual with the entity with legal responsibility for granting the credential or through the use of industry-recognized verification sources. Refers to primary source verification of licensure that ensures diplomates are in good standing with their licensing board(s). Verification can be obtained through individual state medical boards, the Federation of State Medical Boards, or ABMS.
Professional self-regulation
Through an implicit social contract, society grants privileges, resources and substantial autonomy to the medical profession to establish educational standards, assess and ensure the competence of its members. In return, it is expected that the special knowledge and skills acquired by physicians and medical specialists (often through substantial societal investment in their educational process) will be used for the public good.[9],[10]
Professional standing
Professional Standing refers to maintaining high standards of professional conduct in the ethical and safe performance of clinical responsibilities. In the absence of widespread measurement of workplace behavior, we operationalize “professional standing” in terms of the absence of actions by regulatory authorities that signify a breach of professional norms.
Program evaluation
Systematic and ongoing collection and analysis of information related to the design, implementation, and effects of a continuing certification program for the purpose of monitoring and improving of the program.[11]
Regaining certification
Addresses pathways for diplomates to meet additional requirements to regain their certification following the loss of certification (non-participation in continuing certification for an extended period of time, actions by a state licensing board (s), loss of medical staff privileges due to impairment or lack of competence). Regaining certification is different than re-entering practice after an extended period of clinical inactivity.[12]
Specialty
A “Medical Specialty” is a defined area of medical practice that connotes special knowledge and ability resulting from specialized effort and training in the specialty field.[13]
Subspecialty
A “Medical Subspecialty” is an identifiable component of a specialty to which a practicing physician or medical specialist may devote a significant proportion of time. Practice in the subspecialty follows special educational experience in addition to that required for general certification. Two different specialty fields may include two or more similar subspecialty areas. In these cases, the identified subspecialty area might use the same title and even equivalent educational standards.[14]
Summative Assessment
Assessment of learning with the primary purpose of establishing whether performance measured at a single defined point in time meets established performance standards, permanently recorded in the form of a score.[15]
References
Accreditation Council for Continuing Medical Education. (2017, April). AMA/ACCME glossary. https://www.accme.org/sites/default/files/2021-08/11_20210826_revised%20AMA_ACCME%20Glossary_of_Terms%20%281%29.pdf
Accreditation Council for Graduate Medical Education. (2018). ACGME glossary of terms. https://www.acgme.org/globalassets/pdfs/ab_acgmeglossary.pdf
American Board of Medical Specialties. (2014, January 15). Standards for the ABMS program for maintenance of certification.
American Board of Medical Specialties. (2018, June). Amended and restated corporate bylaws of the American Board of Medical Specialties.
American Board of Medical Specialties. (2018). Guide to the medical specialties.
American Board of Medical Specialties. (2019, February 12). Continuing board certification: Vision for the future commission final report. https://www.abms.org/wp-content/uploads/2020/11/commission_final_report_20190212.pdf
American Board of Medical Specialties. (2019). Remediation Task Force.
Caldwell K, Chaudhry H, Johnson, D. (2016). Medical licensing and credentialing. In Stephens KG (ed), Guide to medical education in the teaching hospital. Association for Hospital Medical Education. https://ahme.org/publications/
Cruess, R. L., & Cruess, S. R. (1997). Teaching medicine as a profession in the service of healing. Academic Medicine, 72(11), 941–952. https://doi.org/10.1097/00001888-199711000-00009
Frank, J. R., Snell, L. S., Cate, O. T., Holmboe, E. S., Carraccio, C., Swing, S. R., Harris, P., Glasgow, N. J., Campbell, C., Dath, D., Harden, R. M., Iobst, W., Long, D. M., Mungroo, R., Richardson, D. L., Sherbino, J., Silver, I., Taber, S., Talbot, M., & Harris, K. A. (2010). Competency-based medical education: theory to practice. Medical Teacher, 32(8), 638–645. https://doi.org/10.3109/0142159X.2010.501190
Institute of Medicine (US) Committee on Quality of Health Care in America. (2001). Crossing the Quality Chasm: A New Health System for the 21st Century. National Academies Press (US).
Norcini, J. (2018). Revalidation and recertification [PowerPoint slides].
Price D, Resnick S. (2016). The American Board of Medical Specialties certification system. In Stephens KG (ed), Guide to medical education in the teaching hospital. Association for Hospital Medical Education. https://ahme.org/publications/
[1] From the Standards for the ABMS Program for Maintenance of Certification. American Board of Medical Specialties. (2014, January 15).
[2] Modified from Continuing Board Certification: Vision for the Future Commission Final Report. American Board of Medical Specialties. (2019, February 12). Page 52. https://www.abms.org/wp-content/uploads/2020/11/commission_final_report_20190212.pdf. Originally derived from “Competency-based Medical Education: Theory to Practice.” Frank et al. (2010, July 27). https://www.tandfonline.com/doi/abs/10.3109/0142159X.2010.501190?journalCode=imte20
[3] Modified from Continuing Board Certification: Vision for the Future Commission Final Report. American Board of Medical Specialties. (2019, February 12). Page 53. https://www.abms.org/wp-content/uploads/2020/11/commission_final_report_20190212.pdf. Originally derived from the AMA/ACCME Glossary. (2017, April). https://www.accme.org/sites/default/files/2021-08/11_20210826_revised%20AMA_ACCME%20Glossary_of_Terms%20%281%29.pdf
[4] Modified from Continuing Board Certification: Vision for the Future Commission Final Report. American Board of Medical Specialties. (2019, February 12). Page 53. https://www.abms.org/wp-content/uploads/2020/11/commission_final_report_20190212.pdf. Definition originally derived from the ACGME Glossary of Terms. (2018). https://www.acgme.org/globalassets/pdfs/ab_acgmeglossary.pdf.
[5] Modified from Continuing Board Certification: Vision for the Future Commission Final Report. American Board of Medical Specialties. (2019, February 12). Page 54. https://www.abms.org/wp-content/uploads/2020/11/commission_final_report_20190212.pdf
[6] From Crossing the Quality Chasm: A New Health System for the 21st Century. Committee on Quality of Health Care in America, Institute of Medicine. (2001). To access this report online visit the National Academies website at https://www.nap.edu/catalog/10027/crossing-the-quality-chasm-a-new-health-system-for-the#toc.
[7] From ABMS Remediation Task Force
[8] Modified from Continuing Board Certification: Vision for the Future Commission Final Report. American Board of Medical Specialties. (2019, February 12). See “diplomate portfolio” definition on page 53. https://www.abms.org/wp-content/uploads/2020/11/commission_final_report_20190212.pdf. Definition originally derived from Revalidation and Recertification [PowerPoint slides]. Norcini J. (2018, May).
[9] The principle of self-regulation works in tandem with state-based licensing processes. Self-regulation extends the Member Boards the privilege to determine standards for designation as a medical specialist. Licensure requires that an independent licensing body makes the final determination that a physician is competent to engage in the unsupervised [general and undifferentiated] practice of medicine within a given jurisdiction.
[10] Modified from “The American Board of Medical Specialties Certification System.” Price D, Resnick S. (2016). In: Stephens KG (ed). Guide to Medical Education in the Teaching Hospital (5th Edition). Irwin, PA, Association for Hospital Medical Education, 2016.
Originally derived from “Teaching Medicine as a Profession in the Service of Healing.” Cruess RL, Cruess SR. (1997). In: 2010 ABIM Foundation Forum, Principles of the Social Compact for Medical Education and Training, Leslie Tucker and Daniel Wolfson, ABIM Foundation.
Licensure language reference modified from: Caldwell K, Chaudhry H, Johnson, D. Medical Licensing and Credentialing. In: Stephens KG (ed). Guide to Medical Education in the Teaching Hospital (5th Edition). Irwin, PA, Association for Hospital Medical Education, 2016.
[11] Modified from Continuing Board Certification: Vision for the Future Commission Final Report. American Board of Medical Specialties. (2019, February 12). Page 56. https://www.abms.org/wp-content/uploads/2020/11/commission_final_report_20190212.pdf. Definition originally derived from the ACGME Glossary of Terms. (2018). https://www.acgme.org/globalassets/pdfs/ab_acgmeglossary.pdf.
[12] From the ABMS Remediation Task Force (2021, June).
[13] From Amended and Restated Corporate Bylaws of the American Board of Medical Specialties. (2018, June).
[14] From Amended and Restated Corporate Bylaws of the American Board of Medical Specialties. (2018, June).
[15] From Continuing Board Certification: Vision for the Future Commission Final Report. American Board of Medical Specialties. (2019, February 12). Page 56. https://www.abms.org/wp-content/uploads/2020/11/commission_final_report_20190212.pdf. Definition originally derived from the ACGME Glossary of Terms. (2018). https://www.acgme.org/globalassets/pdfs/ab_acgmeglossary.pdf.
Appendix II: Development of the Standards
As part of its commitment to ongoing quality improvement, in 2018, ABMS established the Continuing Board Certification: Vision for the Future (Vision Commission). This initiative brought together multiple stakeholders to advise on redesigning continuing board certification to be more meaningful, relevant, and valuable to diplomates while remaining responsive to the needs of patients, hospitals and health systems, and others who expect that diplomates are maintaining their knowledge and skills to provide quality specialty care.
The independent Vision Commission represented a broad cross-section of physicians from various specialties and practice settings, a diverse group of stakeholder communities including national specialty and state medical societies, hospitals and health systems, health care organizations, ABMS Member Boards, and the general public. The Vision Commission members assessed the state of continuing board certification and made recommendations to implement a system of continuing certification that better reflects the commitment to professional self-regulation and promotes the highest standards for the provision of patient care.
In response to the Vision Commission’s recommendations, ABMS and its Member Boards created the Achieving the Vision Initiative to design new standards for continuing certification programs consistent with Vision Commission recommendations. Task forces were organized around the themes of the Vision Commission recommendations: Advancing Practice, Information and Data Sharing, Professionalism, and Remediation, all composed of representatives from various external stakeholders in the continuing certification process and ABMS Member Boards. An Oversight Committee and a Standards Task Force were also created to coordinate the initiative.
The Oversight Committee and task forces periodically sought feedback from the Member Boards, external stakeholders, and the public during the development of these standards. A draft of these standards was presented for public comment from April to July 2021. The Standards Task Force reviewed feedback from thousands of individuals and organizations. The feedback collected was highly valued and each draft Standard was revised in some manner to address the comments received. This resulted in a final set of Standards that meets the needs of the stakeholders who possess, use, or rely upon the board certification credential as an indicator of a diplomate’s skills, knowledge, judgment and professionalism.
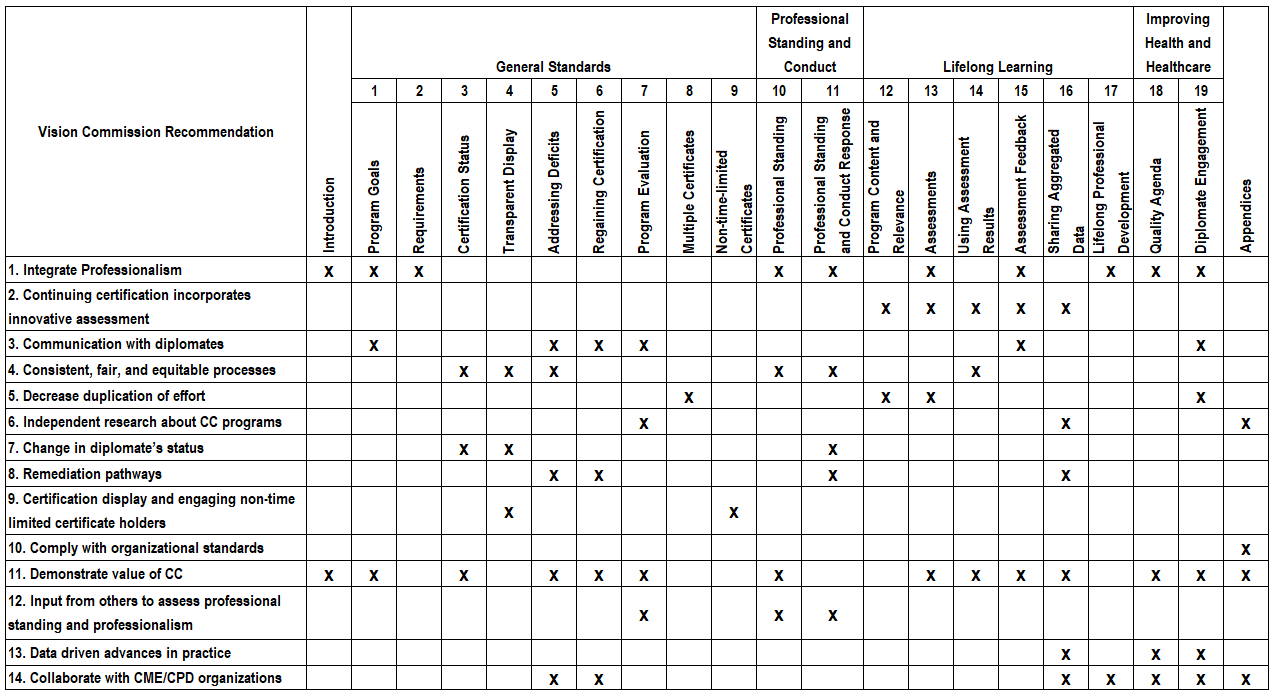
Table 1: Crosswalk of Draft Standards to Vision Commission Recommendations
Appendix III: Design, Implementation and Evolution
Design of Programs Consistent with These Standards
Member Boards should consider designing continuing certification programs that integrate professionalism, lifelong learning, improving health and healthcare. Programs should identify high-priority population and public health needs, frequently occurring harms, and advances in practice within the specialty; this should be done in collaboration with specialty societies and other educational partners.
Once these priorities have been identified, the development of associated assessment, continuing education, and quality improvement activities can follow. These activities should reinforce learning and quality improvement as well as lessen the burden on participating diplomates by taking advantage of education and improvement activities in which they already engage.
As an example, an integrated program would enable identification of strengths and opportunities for learning and/or improvement and facilitate linkages to resources to close knowledge gaps and/or improve the quality of care delivered. Selected learning activities may translate into a change in practice. Sharing aggregated information from continuing certification activities with specialty societies and other educational partners (Standard 16), will assist them in development of targeted learning resources and enable Member Boards to fully integrate activities for diplomates.
Implementation of Programs Consistent with These Standards
ABMS recognizes that it will take time for Member Boards to implement new programs consistent with these new standards. For the new programs to be well received, Member Boards will need sufficient time to communicate with diplomates and other stakeholders.
The revised Standards will take effect on January 1, 2024. Diplomates will be phased-in to Member Boards’ programs as they attain initial certification or complete requirements to continue their certification. Specific phase-in periods will be determined in cooperation with the Member Boards as they begin the implementation process.
Determination of Compliance with the Standards and the Evolution of Continuing Certification
The ABMS Committee on Continuing Certification (3C) will oversee the review process for Member Board continuing certification programs. Member Boards will submit self-assessments of their readiness for change, implementation plans, and a timeline to 3C. This information must include phase-in periods, specifying how each board will meet the new Standards for Continuing Certification. Member Boards will be held accountable to the public, each other, diplomates, and external stakeholders by the review process led by 3C. This review process will reflect a continuing Quality Improvement philosophy that emphasizes the sharing of best practices among the Member Boards.
It is anticipated that these Standards and the Member Boards’ programs will evolve to keep pace with advances in medicine, changes in practice, and local and national quality priorities for population health and health care. As part of the design and evaluation process, the ABMS and the Member Boards should collaborate with external stakeholders to facilitate the ability of independent researchers to examine the effectiveness and efficiency of continuing certification, the impact on diplomate engagement, stress, and burden, and the impact on the quality of health and health care.
On June 5, 2019, ABMS Board Chair Barry S. Smith, MD, and ABMS President and CEO Richard E. Hawkins, MD, wrote a letter to chief medical officers and executive leaders at hospitals and health systems throughout the country. The letter communicated the ABMS policy on the appropriate use of board certification in privileging and credentialing decisions by hospitals, and invited hospitals and physician leaders to engage in a conversation about new approaches to assessment that are transforming continuing board certification.
ABMS believes strongly that hospitals and health systems should be free, without any legal restraint, to consider certification status when rendering a decision about hospital privileges, and trusts that they will make those decisions based on their system’s quality and safety needs. However, we also recognize that certification status is not the only indicator of a physician’s quality, and it has been our policy for decades that it is not appropriate to grant or deny privileges solely based on certification status.
Compliance with ABMS Organizational Standards
Member Board bylaws, policies (e.g., non-discrimination, fairness, due process, data protection), and other organizational structures are periodically evaluated as part of the review of ABMS Organizational Standards. Member Boards are required to adhere to the ABMS Organizational Standards that serve to promote consistency across ABMS and ensure that ABMS Member Boards maintain high standards for board certification.